 Live Music Archive
Live Music Archive Librivox Free Audio
Librivox Free Audio Metropolitan Museum
Metropolitan Museum Cleveland Museum of Art
Cleveland Museum of Art Internet Arcade
Internet Arcade Console Living Room
Console Living Room Books to Borrow
Books to Borrow Open Library
Open Library TV News
TV News Understanding 9/11
Understanding 9/11tv Book TV CSPAN November 4, 2012 4:45pm-6:00pm EST
4:45 pm

is not democracy. and so, once the understand that what we think of as democracy is not what the founders were envisioning it was what people were used to for much of the history of the country that forces us to really look at what we mean by democracy and how we can get back. with slow democracy does is it offers a worldly thinking and a set of principles so that people can find their own policies that work for themselves and their own communities. we have town hall meetings and they worked incredibly well but in california that is in the tradition and there are others people can build on but if they can look and say okay in order to be really a valuable democratic process something needs to be inclusive and the lubber to it and it needs to be empowered. that provides enough of a framework for people to say here's how we can do it in our area. we don't have to have town halls
4:46 pm

we can have oranges and others in california so people can take that inspiration and use it wherever they are and hopefully i think in some ways that can have an impact on the national conversations. rosemary gibson reports on the creation of the patient protection and affordable care act and its recent passage and fiscal affect on the federal government. this is just over an hour. it's a pleasure to be here. thanks to you at st. peter's
4:47 pm

university hospital for the opportunity to be here today. the topic today's health care reform. it's based on the book and the principal author called the battle for health care obama as reform for america's future is a nonpartisan analysis of health care reform and we are headed. i approached writing that book with a question how did this happen. since the time of franklin roosevelt america has tried to have universal health insurance coverage in this country that tried for decades but it failed. how did happen this time? what went on behind the scenes in the deals the for done for the important players in that what went on? what made it happen? with a special ingredients?
4:48 pm

and it america get a good deal we will talk a lot about that today. will health care be favored? will there be less over treatment? for you and future physicians there are many residents in this room today. what will healthcare look like you as a future physician? really important question. finally, did we build and health care reform a sustainable system? we build a house but it will be one that generations will be able to levin. let's get started. last night at dinner we were talking about applying for the underinsured here and they come in with advanced heart disease, and managed diabetes and cancer that has spread why?
4:49 pm

because they've lacked health insurance because it is too expensive and the enormous suffering that takes place because people don't have access to health care. this is a photographic. they provide health care for the uninsured, this has been america's safety nets. this is where people will drive hundreds of miles to receive needed care whether it is a pair of eyeglasses, a sore tooth that needs to be pulled or cancer treatment but can't afford the follow-up care this is where you go. this has been healthcare in america for millions of people. so the decisions on what to do about it this is a picture of blair house in washington, d.c.. the white house summit in early 2010. democrats and republicans
4:50 pm

together debating and quarreling over what it should look like if it should even happen at all. in the battle for health care will continue. today health care reform is the law of the land and it's been signed by president and passed both houses of congress. the supreme court affirmed the constitutionality of the mandate last month but still the battle will continue. republicans have vowed to repeal what to read if not the have vowed to prevent it from being funded and there are many substantive issues that remain to be addressed. we still have a shortage the imbalance between primary care and specialty care remains a huge challenge are there enough to take care of the 32 million people who might have health insurance coverage because of health care reform? and then we have a surgeon the elderly population as the boomers turn on medicare for 30 million people over age 65 will be on medicare in the next
4:51 pm

25 to 30 years. do we have enough doctors and nurses to take care of them? health care reform couldn't fix everything. but there is still a lot to be done and the battle will continue. so this presentation is a non-partisan look at health care reform. the focus would be on the two main areas, coverage and cost. we can't cover it now because it is such a huge bill. the bottom line is if you want to build a health care reform provide a good foundation. will that be a around and support people for good care and generations to come so in the future the residents that are here now 40 years from now look back on it did we do health care reform right? that's the question. there will be four parts to the presentation this morning. it did health care reform diagnose the right problem? we know how important getting an accurate diagnosis is. did we do that as a matter of public policy? the second question is what will be covered and what will it
4:52 pm

cost. third we will focus on what is health care reform mean for you as future physicians and for those of you that are currently practicing. and finally, where are we headed from an economic point of view and fiscally can we sustain financially the systems that we are creating? and if we can't, what should we do about it and start doing now to fix it? he hid the health care diagnose the problem correctly? they diagnose the problem as a lack of health insurance. there are a to 50 million people that suggest they don't have insurance. and so the solution that has been prescribed, the treatment order is let's have more insurance. and so now to 60 million people will have access to private health insurance coverage. many of them with subsidies we will talk about that in a minute and up to 60 million people could have medicaid coverage.
4:53 pm

one of the reasons that so many people could not afford to, couldn't get insurance because they couldn't afford it and that is because health care costs are too high. we are going to drill down on that in the next few minutes. this is to be published in the archives of internal medicine earlier this year that looked at the cost data for uncomplicated appendicitis in the state of california. the researchers have access for all of the hospitals in the state and the median cost of a hospital bill to treat uncomplicated appendicitis was $33,611. that amount is 75% of the annual per-capita income in the state of california which was $44,481 in 2011. what's especially interesting is the range of how much the hospital bills were. at the local county hospital it was only $1,500. at other hospitals it went up to
4:54 pm

nearly $183,000. some of the higher cost hospitals according to the study of the for-profit institutions. how do we sustain this? is it sustainable? i'm writing a book on medicare presently in the had the pleasure of interviewing and 65-year-old gentleman from kentucky that went into the hospital for one night for a procedure he wanted to keep private but he said he needed an operating room and the chances are she might have had a pacemaker orie defibrillator implanted. he got a hospital bill for $244,000 for that one night in the hospital. and that's about the cost to buy a house in this community. in fact you can buy houses cheaper than that in his community. he was on medicare and medicare people the $18,000. she would call the hospital and see what happens if i do have insurance? he said well, we will still make you pay it.
4:55 pm

i recently did a radio interview in washington, d.c. and a woman called in and she said that her husband had gone in for treatment for kidney stones. he had two of them and they got a bill for $62,000 for each one. this is the reality of how much health care is costing and this is why we have health insurance creams that keep spiking. in 2011 a drug company gained exclusive rights on the upper jester and shot to prevent premature births. you used to be about to buy it for $10 an injection. when they gain the exclusive right the increase the price to $1,500 per injection for a total cost of $30,000 per pregnancy. it's unsustainable. and this happens in the united states because there's nothing to stop it. there's nothing to stop the price increases.
4:56 pm

in this case the american college of obstetrics and gynecology pushback. the issue a statement that said the u.s. of consent system cannot afford the cost at its current price without significant negative repercussions. in this case the company backed down. this is the exception rather than the rule and individual patient still have the power to put pressure to reduce their hospital bill econ so we have a problem of one controlled prices in american health care at the time when 32 million people will be getting coverage. we also have an interesting situation a recent study in the archives of internal medicine was a survey of physicians primary-care physicians 42% of them believe their patients received too much medical care. 25% of them believe that they themselves provide too much medical care.
4:57 pm

the good news is about 75% of the surveyed said they are interested in learning how the practice compares to other doctors so they can have unnecessary medical treatment. as young residents you have the opportunity to do that and i'd sure with the leadership you will learn how to do that, and you should. he would be aware of the american board of internal medicine foundation choosing the campaign to encourage doctors to provide the care people need and not the care they don't read the issue the top five lists coming out for 27 different specialties within medicine as things that we can do less of and have really good care for patients. here are the top five in internal medicine you might already know them from the previous presentations but i will run through them very quickly. imaging for low back pain often overused. let's do watchful waiting for the first four to six weeks when there are no red flags. don't do the blood chemistry panels and a symptomatic healthy
4:58 pm

adults. don't do the annual electrocardiograms come again and a symptomatic patients. don't do the bone screening for osteoporosis in women under age 65. these are recommendations coming from the evidence from primary care physicians. we will talk more about this later about what we can do to try to curb the extra will rise in health care spending so we can have health care reform that lasts for generations to come. this is a medical index of the annual cost for a family of four to the medical care. and note in a 2012, $20,728 has been rising at thousand dollars a year. you can see that. that's where we are not health care today and there is nothing to stop that trajectory. meanwhile the median family income in the u.s. in 2011 was
4:59 pm
$60,000. so how in a family of four the average annual spending is $20,000. how do you do that. and are there enough federal subsidies. is there enough money in the federal government to keep subsidizing that? while we were writing the battle for health care i listened to an interview on the abc nightly news. the secretary of health and human services kathleen sebelius was being interviewed in the context of the stories the were being reported about tremendous increases in health insurance premiums that individuals were having to pay 20, 30, 40%. and i found the question and answer really quite remarkable. the question that was asked by the interviewer is what should people do if they get an increase in their insurance premiums at 20, 30 or 40% and they can't afford it? and this is after health care reform and the most remarkable answer which i quite frankly was not aware of until it was said
5:00 pm

so starkly her reply was they should contact the governor of the state and state legislature demanding that all law be changed. .. the gulf of mexico. and these pictures like this were seen around the world of the oil coming out of the earth, and there was no way to stop it. day-by-day by gay people watched this around the world.
5:01 pm

no way to cap it. finally, the engineers were able to cap it. i cannot help making the comparison with healthcare. there is nothing to stop it. it keeps coming and coming, and there is nothing to stop it. just a word about medicare. one part of health care reform law that has brakes on it pertains to medicare. there are a number of other provisions, adding preventive benefits for annual mammograms and : naskapis without co-payments, closing the doughnut hole for prescription drugs, all good things. and that is -- here is where we're headed in medicare. this is a -- from the medicare trustees' report that reports on the financial state of medicare. it starts in 1967. this is a data for how much the average person who is over 65 and collecting social security. let's take someone who has earned $50,000 per year, the average wage or the course of their working life.
5:02 pm

they retire. and you have to pay for medicare. it's not free. you have to pay premiums and co-payments. you paid for part b, which is dr. sturgis and part b is prescription drugs. end in 1967, two years after medicare was started, the average person on social security paid 6% of their social security check just for physician visits. there was not part deep. so 6% of their social security check. in 2010 its 27%. in 2035 is going up to 40%. twenty-five, when the young people in this room, when you are in your eighties, you will be spending 46 percent of your social security check just for physician visits and prescription drugs. does not include the cost of hospital care, the deductible, nor the copayment you have to pay. again, these projections. this is very sobering.
5:03 pm

so in the health care reform law there is recognition that medicare, we need to find a way to address that cost to victory. there is a provision for an independent in advisory board to be set up with 16 -- 15 members appointed by the president and confirmed by the senate to recommend ways that medicare can keep spending in check. now, there is one thing that can't believe it or not, president obama and rush limbaugh agree on. they agree that medicare is unsustainable as it is now. they agree on something. it must be true. here is what president obama said. the u.s. government is not going to builds of for medicare on its current trajectory. the notion that somehow we keep on doing will we head doing in its okay is not true. rush limbaugh said, i'd like the idea of letting medicare collapse. there will be any medicare free of fix it. it is not sustainable. so independent payment advisory
5:04 pm

board concluded in the health reform legislation it cannot change eligibility, ration care, raise premiums. if congress does not like the recommendations, it does not have to implement them. congress does have to find an equivalent amount of savings to pare back medicare spending. the independent payment advisory board has been targeted for repeal. very powerful forces. and in part because -- and they're is a consistent pattern in health care reform and how the deals were done. in the curve on any revenue, any effort to curb that revenue, they want to stop. so just as there is 2 million people have insurance, the health care industry will begin 302 million new customers. that's lots of revenue, and they don't want any impediment on getting that revenue. what is so interesting, the year that the health care reform law was signed the "wall street journal" reported its annual ceo
5:05 pm

compensation survey. they reported that the highest median compensation of any sector of the u.s. economy that year was health care. it was not the banking industry. it wasn't the oil industry. it's health care. i'm also mindful of during the financial crisis charles prince, head of the seven the music stops things would get complicated, but as long as the music is playing, we have to get up and dance, and we are still dancing. i sometimes feel that about health care. living trajectories, and where are we headed? so the question remains, is health care reform bill to last? what do you think? lets talk about the cost and coverage provision under health care reform. who will be covered under the patient protection and affordable care act? or will it cost? the good news is, up to 16 million low-income people may be covered under medicaid, the
5:06 pm

joint federal-state program. maybe because there are a number of state governors you are not inclines to expand medicaid. at think it is more for political reasons. they also have some very serious budget situations. i suspect there will be a lot of pressure from hospitals and others in the state that will wear down that opposition. so it's that clear all 16 million projected people will be on medicaid. in new jersey its estimated at 400,000, 450,000 people, some of the people will come to your clinic who are uninsured now will have insurance. that will be a good thing. so what is this individual mandate? it requires almost everyone under age 65 to have insurance either from their employer or for medicaid or private insurance. and if they don't have it they will have to buy it, and the individual mandate applies to those without employer coverage for medicaid, and that will affect an estimated at
5:07 pm

60 million people, and they have to start getting insurance starting in 18 months, january january 2014. it is not received a lot of attention, the number of of cost. there has been a lot of talk about subsidies, but how much will it cost? so the kaiser family foundation as a wonderful calculator. just estimates and projections based on data from the congressional budget office. and they report that a 45 year-old head of household with an income of $46,000 per year will pay $2,600 a year for insurance in 2014, and that's subsidized. in addition, they will have maximum out-of-pocket cost of more than $4,000. the way the subsidies are structured the benefits are different. a 60 year-old person earning $48,000 per year will pay $10,000 for insurance in 2014. plus out-of-pocket cost up to
5:08 pm

$6,000. i was surprised at how much that was. so what is in exchange and how will it work? people will be able to get their private insurance on an on-line exchange. there will also be allowed to access it by telephone. it will provide information to help consumers stop -- shop for a state approved health-insurance plan. like the travel website, like expedia, it will all be there. you can select your choices from that, make it a lot easier than what is now. you might have heard about the penalty. to have to pay a penalty of that up by insurance? in two dozen 16 the penalty will be $695 a year or two and a half percent and come, but there will be exceptions. you will be exempt if you have financial hardship for religious reasons and others who will have to pay the penalty.
5:09 pm

so as health care reform moves from the supreme court to the court of public opinion, will people buy insurance? it will labial to afford it, even with subsidies? by the panel is strong enough to encourage people to buy insurance? you can imagine that people with the serious illness who have not been able to buy insurance because they have been excluded, there will be delighted at the prospect, so relieved they will sleep better at night that there will be able to have insurance and will be happy to buy it. others may feel differently. healthy people don't enroll and only the sick people in rural, what's going to happen to those premiums? if you have only sick people, they're going to go even higher. there is no enforcement of the penalty. there is no lanes on your property or garnishment of wages so even though we have come this far, still many unanswered questions and uncertainties. what about employer provided
5:10 pm

insurance? that will partly affect most of you in this room will are fortunate to have it. how many of you have insurance? so what will employer provided insurance costs? what benefits will it offer? well, will employers continue to provide insurance? most employers will pro we continue to provide insurance, as they are now, but it's changing. i'm sure you have seen the changes yourself. you're paying more a very come for health-insurance. people are getting fewer benefits. the deductibles and higher. i call it the swiss cheese. health care insurance has become like swiss cheese. it has lots of holes. more holes, unless she's. here is data from the kaiser family foundation and h. r. et. on the bottom line you will see the growth in employees' income from 1999-2011. so people's incomes have been
5:11 pm
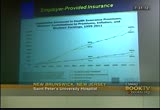
growing over that time frame by about 50%. it's a cumulative increase. but then look at the top line. that's how much people are paying more for health insurance. the increase in their health insurance out of pocket for employees is 169%. you have a huge gap. what it means is incomes are not rising anywhere near as fast as the cost of health care. in d.c. that trajectory. it's still going up and up and up. as you look in the top right corner right here, while insurance is going up, employees are being asked to pay a higher share of it, and that is reflected a year and a slide. if you work in a company with 3- a hundred 99 workers, the topline here, you will see that 29 percent of employees of pain to thousand dollars deductibles
5:12 pm

before their insurance kicks sand. like it that growth trajectory from 2006. 6 percent and much higher in 2011. so there will be insurance, but it will have a lot of holes. there is a penalty for employers if they don't provide insurance, depending upon how large the employers are. employers with more than 50 employees that do provide insurance and have at least one full-time employee who receives subsidies from the insurance exchange we will pay a penalty. $2,000 for full-time employee excluding the first 30 employees but the businesses have already calculated that is cheaper for them to pay the penalty and it is to pay insurance. what's going to happen? this is the trajectory of all firms offering health benefits for 1999-2001. the researchers are not sure about what causes that the ec here.
5:13 pm

you see the overall trajectory is moving downward. and i predict that will continue, particularly among small employers. what they may do is just offer, like we have done with retiree benefits to move from a defined benefit and defined contribution a set amount of money and then you can go get your insurance. i predict that this will happen. what about states and medicaid? the medicaid expansion, and the federal government will pay 100 percent of the cost of the medicaid expansion from 2014- 2019. beginning in 2020, that will change and states will have to pay 10 percent of the cost. if he had been reading the news, if you have time, you will see that california and new york both headed by democratic governors, have had to slash medicaid budgets because the overall state budgets are under tremendous pressure.
5:14 pm

a former state medicaid director in california under governor arnold schwarzenegger said this, medicaid provides care that is invaluable, but it is reeling under its own weight. states are now being asked to implement the largest social programs as medicare and medicaid began. medicaid is falling apart as states cut benefit as enrollment freeze increases because of the recession. we are still seeing the aftereffects of the recession. a recent report came out of the state of state finances two weeks ago. a very challenging environment still. health care reform, what does it mean for u.s. physicians to back will be different? what will life be like? the good news is more of your patients will have health insurance having dinner last night, the doctor was mentioning how when he was a round in 1955 and medicare and started, basically had to close the clinic because older people no longer needed a free clinic for
5:15 pm

the uninsured because they at medicare. here there will still be uninsured americans, but there will be far fewer of them, and that's a good thing. what about primary-care? access to primary care will be more challenging than ever. the way i talk about it, health care reform is like building a house without a first floor. there are some provisions in the health care reform law, terms and may have heard call patients entered medical homes which are wonderful things, but they are not enough, and not enough primary-care physicians or nurse practitioners to be able to the handle the number of people who need care. in fact, in many hospitals around the country, if you call up to get an appointment with a primary care physician, you cannot. we will be having 302 million more people, to the system. and people on medicare, while we close the doughnut hole for
5:16 pm

prescription drugs, the number of geriatricians is actually shrinking. who is going to take care of those 35 million more people who will be on medicare in the coming decade. who's going to take care of them? who will coordinate their care? as future physicians, you will be practicing in a professional team based care. we will be expected competency. practices we will need high functioning teams comprised of physicians and advanced practice nurses, clinicians and it you will be expected to demonstrate competency in working in a professional team. this will be part of your maintenance and certification assessment. this will be an expected competency because we have to work in teams to manage all the care. the other thing they you will be seeing is down more pressure on physician payment.
5:17 pm

as all those cost pressures keep escalating, there is only a few ways to cut that, and that is to keep payments love. we are already seeing that, and we are seeing, as a consequence, demands are increased. see more patients in a shorter amount of time. that is very dissatisfied to u.s. physicians, and very dissatisfied to patients. on the flip side, what's going to happen is an increase in volume. we will be working faster and faster. so the question we have today is, how do we ensure that health care reform is, indeed, built to last. how are we going to ensure that the health -- house that we have built is going to be around for generations to come? if current trends continue the debt are really clear that we
5:18 pm

just cannot continue, and this would have happened whether or not there was health care reform if anything health care reform may exhilarated because we have more people using more care. this is going to happen even without health care reform, and this is not a democratic republican issue. everyone bears is possibility. so what happens if we don't act? and economics at. you may have heard about the national debt. the national debt is how much the federal government owes the people who have lent it money. in 1985 the united states was a net creditor to the world. we have -- we used to loan money to countries. here we are in 2012, the u.s. has gone from net creditor to a net debtor. we don't want people money anymore. we have to borrow from them to pay the bills.
5:19 pm

so when you see medicare patients, and those bills go into medicare, the federal government does not have enough money to cover its bills. it has to borrow money from countries like china to pay those doctor bills and hospital bills. how much debt as the u.s. have? , presently the total debt is $16 trillion. it's hard to get your hands around what is 16 jillion dollars. here is what $1 trillion is. if i paid the doctor a million dollars a day since the year one, says the year jesus christ is born, that would not total a trillion dollars. and we have 16 of those. that is how much debt the u.s.s. and so when you hear the debates in congress which will come up again about raising the debt ceiling, that is what this is all about. are we going to allow the
5:20 pm

country to keep borrowing more and more and more? and it is something that i hope never happens, but if we don't act now, at some point, we of looking at what is going on in europe and the eurozone countries, places like greece and spain, they cannot repay debts. they're having to ask for bailout money from eurozone countries and the international monetary fund, have never been the united states ever gets in a position, the international monetary fund is already monitoring health care reform because the united states is a member of the international monetary fund. so that is the debt situation that we are looking at is a country. so readily begin to change course? and that is where all of you, and, especially those of you who are future physicians who will be taking care patients. what can you do? the institute of medicine
5:21 pm

estimates that about 30% of all the money spent on health care in the united states is wasted, meaning it does not add value to the care of patients. it does not improve their health so what is included? it includes overuse. it includes inefficiency. it includes fraud. we will talk about each of these and how much 760 billion is close to that jillion dollars. we waste that every single year. if we can take that out of the system we will be -- even a portion of it, we will be in really good shape, and you a bill to house the health care reform that will be around for generations to come. it will depend, in part, in part, on you. not alone. so what? that stroke you use every day to
5:22 pm

order tests and prescription drugs. very, very powerful tool you have in your hand. as mentioned earlier, the choosing lies the campaign, 27 medical societies that are developing top five less or are developing them of things that we can do a lot less of or maybe stop doing all. in addition, there are other procedures and surgery's that have been well documented in the medical literature is being overused. heart bypass surgery, angioplasty, back surgery, prostatectomy, antibiotic use, all over used. in september of this year the joint commission which accredits the nation's hospitals or many of them, will be hosting its first meeting on over treatment, and there will be looking at a number of these topics and trying to come to consensus on what it can do as an a creditor of hospitals to encourage hospitals to reduce unnecessary
5:23 pm

treatment. i think we have a moment in time now with health care reform that if we had unnecessary procedures , stop doing them on people who don't need them. use the talent and skill and resources on people who really do need them. if we can make that switch now, everybody will be kept intact. maintenance of board certification, if you will be seeking board certification in the future. i see your heads,. 2015, appropriate use will be part of minutes of certification . knowing when it's appropriate to do imaging for low back pain screening for osteoporosis. appropriate if you do oncology so that third round of chemotherapy and when is there no evidence that it will actually benefit the patient.
5:24 pm

what -- when is angioplasty appropriate and not? this is what you have the opportunity and will be required to learn. it's a good thing. we can keep the system all for everybody needs it. what is overuse? it was defined by the institute of medicine as when the potential for harm exceeds the possible benefits. so this is not about rationing. this is not about cost control. this is, in fact, about good care of the patient. i have been continuing to work on over treatment. i was here two years ago to talk about the book i wrote called the treatment trap. and i'm happy to say, now, it was a lot more to address this issue of over treatment. here is what some patients are saying about their experience. a colleague and i used to work with said, i have been getting in the kgs my annual physical exams of those 27. of 41 now. i don't know why been getting
5:25 pm

it. i have no heart disease. my husband gets one, too. it i spoke with this person recently and she said, you know, i went and talked to my doctor, and i don't get those anymore. the same with my husband. they're not medically necessary. here is another one. i get a chest x-ray every three months for my doctor. i don't have any underlying medical condition. next among going to ask my. this actually came from a state legislator. i give a talk at the council state governments recently, the east coast regional conference. it was how we really have to address this issue of overuse of we are going to have a sustainable system and a house where everyone can 11. and he brought this up. he said he was going to go back to his doctor and say, well, gee, why am i getting this to back and think of the radiation exposure. who is counting that? do you even know how much it is? we are not tracking it, and we
5:26 pm

probably should. here is another one from the patient. monies were hurting. i went to a well-known of the pd surgeon. he said he could do surgery. he did not talk about me or my situation. at left end on a personal trainer help me strengthen muscles. i'm much better now. so we are seeing informed and educated people good, informed decisions about the use of health care. is that everybody by any stretch, but at least we're beginning to see it, and rehearsing good doctors have good conversations with their patients about the appropriate use of resources. that is what the choosing campaign is all about and that's why i'm so delighted that you, as residents, will be learning, choosing wisely is part of your curriculum.
5:27 pm

better outcomes, better care and it cost less. abundant opportunities to do this. the way i think about health care, as how we deal with food. on the one hand we have an obesity epidemic that is off the charts. people eating too much food, the wrong kind of food, and at the same time we have pockets of communities where people are malnourished. we have this extraordinary imbalance. the same is true in health care. pockets of people who are getting too much medical care and yet we have people who can get what they need. if we can reduce the overuse and put that to good use for people who really needed we will have enough to take care of everyone. we have that opportunity to do it now. we have to get started. we don't have much time or money to waste. that was the topic of the book,
5:28 pm

the treatment trapped, overuse, out of the curve it. finally, here is a fact but i found so interesting. the fbi has done an estimate of how much fraud there is in health care. i began to look at this and give a talk at that health care anti-fraud organization. about 10% of health care spending, the fbi estimates, was lost to fraud. the extent of it and the sophistication of it is enormous . if we take 10% of health care spending, that's over two and a half million that we spend, lost to fraud. that amount of money will cover every single uninsured person in america. just reducing that. the health care reform law
5:29 pm

includes provisions to curb it, but the last very important steps was a far cry from what we do take that out of the system and use that money for good care for people in need it, the people who come to your clinic. we have to preserve and sustain. the only way to do that is take up the things that don't add value and use those resources in the things that do have value life. what can you do, as physicians and nurses? you can ask yourself if the test procedure you are contemplating will do that personally get. today agree? the good news is we are seeing more and more consensus, although there is a lot of
5:30 pm

different points of view. i will leave you with this code. it's from my of my ghandi. the poorest and the weakest man and ask yourself if this step you contemplate is going to era be of any use to him. will he be any better off because of it? your doubt and yourself on the vote -- melt away. that is so we can make health care sustainable. it's how we can make health care reform live for generations to come, to serve everybody so they get the care they need, the care that will sustain them and bring them happier, happy lives. thank you for all you do. and happy answer questions. [applause]
5:31 pm

you have to go to the microphone so everyone can here because we're on tape. >> zillow. good morning. >> good morning. >> it's nice to hear you again. >> zillow -- hello. this talking point might be collapsing under its own weight. the health care system might collapse. as you say, but on its way to collapsing there will be a lot of avenues that materialize in this global open world. even the health care might be exported. and people might even go, seeking health care elsewhere. knowing all that, already we're
5:32 pm

seeing the globalization on the trade, lots of the industry's growing abroad. allow the people are missing out on employment and likewise health care. and it seems that there will be a lot of pain along the way because this particular part that is going to be so troubling, unregulated, practices might crop up along the way. we'll have to deal with all those. one of the things that cams to mind is the way we're taught. at that school we learned that indications of this command occasion of this operation, indication of that operation. this treatment of that treatment. then when it comes to take care of a patient we tend ted think
5:33 pm

the same way. an operation. by the way, a surgeon. i have an operation to offer you. nothing else was talked about for that patient. the patient left, rightly so. so the mindset has to be changed that as we learned with a single patient what is the treatment, along the way not particularly the most expensive treatment for most rewarding treatment for yourself, i don't think that is taking care of the patient's welfare. so i leave you with that part. the medical establishment has said particularly at the met school level in fact, i taught myself.
5:34 pm

>> you mentioned the word disruption. because of a fellow, federal officials are required to report at a certain point when the medicare program reaches a certain fiscal situation. i will go into all the details. but since the administration of george bush and more recently with the obama administration, federal officials have issued from the morning's about medicare's financial state. and they use the term disruptive consequences to society if we don't fix this long-term trajectory. so you're right about that. that me also say something about globalization. the privilege of speaking of the british medical journal health care improvement conference in
5:35 pm

april on the evidence of overuse translating its improvement. asked his audience of people there from around the world, countries represented. and not sure there were all there at that particular session. i ask them, have you or someone you know ever had medical care that the was unnecessary. all these hands went up. as the nominee reside outside the united states command of his hands were not. i was surprised when people came up after words to say, finland, germany, uk, australia, new zealand. we are seeing in the emerging markets in brazil and india, evidence of overuse. this is a global phenomenon that we will have to tackle. provinces in canada 41 and 42 percent in some provinces of the state budget is health care. if you're doing that in a spending money on education, infrastructure, investment in society, technology. it's an enormous issue pretty tacky for your question.
5:36 pm

>> hi. >> hi. i'm debbie goldstein. i am a gastroenterologist, but i have spent a lot of time in primary care as well. i could spend an hour counterpointing and raising. there are so many issues. it is infinite. i wanted to make a couple of points. that is, the first thing is the whole issue of primary care. the primary care physician is being asked to be the foundation the primary care physician has the most responsibility of any other position. they have to know everything. they have to know what the right and left hand is doing. they have to coordinate. there responsible for everything that they refer people to. they have the least amount of time. there the ones that have to talk to that patient who went to the orthopedic surgeon and really could have been talking about
5:37 pm

going somewhere else for palliative care. they can't do that because they have to go faster because they have to see more patients. and its crushing. it is crushing. and there is no incentive for people to become primary care physicians. the get the least amount of money, have the most amount of responsibility, have the biggest burden for lawsuits, and that brings me to the whole issue of the fact that there is an imbalance. this imbalance that we have, and i really don't know behind closed doors when the whole obamacare, 50 billion pages was implemented, but i have to believe as a physician out in the trenches here that there weren't enough of us in their helping to formulate the plans, and i feel that, you know, just from my god, from my soul, i
5:38 pm

have to believe that because all of the people who employment this plan, all the congressman just happen to be lawyers. because of the fact that we can't control health care costs, part of the overuse of health care has to do with the fact that we are shaking in our boots have the time about being sued for things that we should have to be sued for because using clinical judgment and using standards of care just isn't good enough sometimes because when the lawyers are breathing down my throat we still have to worry about the time that we have to spend in a court room for frivolous lawsuits that will take us away from our patients. and even if we are found to be not guilty, we spend time, away, lose money. our patients suffer, and the lawyers are laughing all the way the bank. this same thing happens. and then have a close because i know of going on and on like a
5:39 pm

mad person. the other thing, as long as you have political action committees that are powerful and the political action committees are powerful. so what did we do? we said, everybody has to have health insurance. so this ceos who are making all the money and you talked about of laughing to the bank because now everybody has to have health insurance. there is no competition across state lines. we have lost the sense of competition to make a product that gives good health care that is going to provide people with the care that they need. instead we have -- we have, you know, we have people having $2,000 of deductibles. it never did any health care insurance at all. premiums going up. no competition. if you could pick, go online and pick any health care insurance product in the country, well,
5:40 pm

maybe we would have competition and people would care about providing a good product. maybe they're would be could insurance, and maybe those ceos will have to take less of the bonus. so we're talking about fraud and such a huge magnitude that it has to be rented out. you know, we just have a lot of work to do, and a lot of it has to do with government. >> well, thank you very much for your comment. i think it reflects the views of a lot of physicians. [applause] the ama in the end came out in support of the health care reform law despite tremendous opposition. so the physician community was divided when it came to whether or not to support it. in that division up continues. at inky make a good point. the patient's perspective. did health care reform designed a system that was going to be good for patients? in the battle over health care
5:41 pm

we take a look at the prize bulls. the toxic assets in health care. drugs ago on the market and then off because they're found to be harmful. we have a lot of too big to fail. a lot of, you know, financial interest a stake that makes it very difficult to change, and i think that's a good relationship between the patient and physician, i'm not so sure that health care reform was built around that, in the stock for doctors, and as luck for patients. thank you. >> can you comment and also address how the health care reform can addresses this issue have the recently published, about 50% of health care cost comes the last two years of life and guess which say leads the way in the dartmouth have this report? new jersey. >> major secrets in jersey. >> okay. >> can you comment on care at the end of life, cost of the end
5:42 pm

of life, and how the new health care reform we will address that? >> well, as you know, there was a attempts to put a provision in the reform law that would allow medicare to pay for a conversation between a doctor and patients about serious issues that could -- of life limiting illness. and suddenly we have this term called death panels that cropped up. took that provision out. the intention of that provision was to recognize that when patients are seriously ill, has commented earlier, seven minutes is not enough time to talk to your physician when you're facing a life flamingo must and have a bad diagnosis. the intent of that was to really create a space and time for what i call this a conversation about what people's choices are, what's important to them so we try to, for political
5:43 pm

reasons, i believe. you know, i spent 12 years at the robert johnson foundation. it started when a major study came out that was published showing how poorly we care for people at the end of life. and so we launched a major initiative, and we started to help hospitals and physicians and nurses establish palliative care programs and house bills, which is a good thing. people can get the care that they want. so while that has taken off and we have a specialty, the question remains how come divided care costs keep going up and out. on the other side of the equation, our families who are deeply, deeply troubled about what many of them, not all, but
5:44 pm

many are deeply troubled. that will rely on physicians, future generations. i would love to hear your thoughts on what we can do to make sure people get the care that they need. public expectations. we think there's a cure for everything. if you turn on television dramas he think we can work miracles. we sent the public a steady diet . there is a cure for everything. every test known to mankind can and should be done. we created this in marriage for the public to believe that more is better and how we begin to reverse that. that is what the campaign attend to do. one of the things we should stop doing in chemotherapy and a certain conditions.
5:45 pm

so i cannot agree with you more. it is very tough politically to do, but for the first time i have heard patients and families describe what they see their loved ones going to end terrible terms. posttraumatic stress. the intensity. and yet the messes desire to want to do good. also, we need and wisdom to know when to stop. consistent with the preferences of patients and families. thank you. >> i think this is probably an unanswerable question, but is there any reform on the actual cost. it is impossible to get your brain around the cost of medicine. it cost $303,000. and so what does it cost?
5:46 pm

of the hospital can sustain itself based on what they get, what does it actually cost? >> i think it's a great question i would hope that the yen physicians in the room and everybody will start asking what it costs. i know a wonderful physician in the midwest who heard the talk in washington not long ago about how physicians need to be good stewards of resources. and so he went back home to his hospital. he has the financial people to go to the inventory with them in his operating room to find out how much of those things cost. he had no idea. turns out, he was surprised. $700,000 or the supplies and equipment in that inventory. 10 percent of it was expired. he -- i really only need
5:47 pm

$295,000. the enormous savings. this just one operating room. so then he went to the ceo. imagine if we did this system live. because gated tickets in billions of dollars. you don't want to era have a ton on the basis of price. we have done these things. let's just do it. we all need to begin stewards of resources. simply asking a question. now we're seeing more try spencer -- price transparency begin to come out. patients go. they have no idea. they think they're going to pay $1,500 for our colonoscopy. you add this and this in this. beginning to see mark price transparency, but that is no guarantee we will see press him down. i think it's asking questions,
5:48 pm

simple questions. how much is that cost. a good place to start. >> i'm of 40 medical students. my question has to deal with more about medical education and the cost of it. i go to one of the most expensive medical schools in the country. and that kind of goes with what dr. goldstein earlier. were coming at a medical school with such a high amount of debt. that kind of changes the opinions of students. what deals should i go into? how was the same myself in the future and pay off my dad and have a good living. so already, the way we get our loans, subsidies, i think they've taken some of the way this year. what is being done about that and but 32 million people, no more and more medical schools are opening up. how are we able to provide and sustained for the cost of
5:49 pm

education and producing one position more and more i feel requires a lot from society, college, medical school, and then turning. so your thoughts on that. >> well, thank you for asking a question. i think we should ask the same issue. what does it cost and why is it cost that much? on what basis do we decide that it should -- that it costs as much. think what we have a medical education, the education college costs going up and health care costs going up. we have the perfect storm of health care and education coming together. you fall right in the middle of the storm, you and other medical students. and i don't think that there is any answer for that. health care reform, the provisions. that is not an answer. the reality is health care reform did not fix that.
5:50 pm

thank you. we have one final comment. >> i am a urologist. i sympathize with the medical students played. the current educational system, and the debt burden that they have. it does not lend them into primary care all, and this is what they need. the system needs to be steered in such a way that it is incentive enough for some sort of leapfrog cost of education in the system. otherwise we will end up importing doctors, specifically here for primary care. i think that is the avenue that the country will have to take. >> i think that is what happened to geriatrics. the lowest paid of all of the specialties to my belief, within medicine. 40 percent of fellowships are
5:51 pm

unfilled. it's symptomatic of that. many foreign medical graduates that are national medical graduates come in and do those fellowships. they may not have the same. so health care reform only fixed part of it. there are many, many other things that need to be done. thank you very much for all you do, the care you provide. [applause] >> tell us what you think about our programming this weekend. you can tweet us, @booktv. comment on the facebook wall or send us an e-mail. book tv, nonfiction books every weekend on c-span2. >> from vermont, i tore. here, repair benedict start of the stores' plans to of longstanding role, the impact of commercial competition, and how
5:52 pm

the store has survived for nearly 40 years. >> will we are well known for his are squeaky floors. we have these wood floors that make a ton of noise and our customers love it. we, you know, it's a little bit lost on us why this is so wonderful because we listen to it all day long, but it is the character. we are not a super slight box door kind of look. i think people, i think the squeaky floors represent that. it is just kind of a real old kind of store. you don't get a hell of communities anymore. independent bookstore, here since 1973. i have run the store since 2006 along with my husband. it was opened by michael katzenberg in 1963 across the state, and it has been part of
5:53 pm

the community ever since. they moved the store after a flood in '92 when the all-star have flooded. it was time to expand and starred in the first base. they moved here. their conduct is really a community bookstore. people have been coming here since the beginning. kids have grown up here. it's definitely like being part of that community. i don't think you will find too many towns of 8,000 people that support three bookstores. at one time we have five. mostly closing around the country. a lot of them are closing. close doors of been in business. changes of ownerships and retirements and things like that . this is a community that values
5:54 pm

books, values reading. we have a lot of writers. it is also a community that beyond that values independent stores. it really makes a huge difference and pines and a blood coming to town that out of its of the year. there are certainly borders and barns and nobles. this community long before the local and shop local movement started, this community understood that if you wanted to have a bookstore you have to shop at the bookstore, not go to barnes and noble and say that you loved the story, which i think is a problem. people definitely say they support their stores, but when you're purchasing elsewhere you're not release supporting the store. this community really understood that from the beginning, and we had people coming here all the time.
5:55 pm

alexis upon line. i want to buy from you. we hear that all the line every day. i lifted up. i would never buy. we appreciate that. that attitude keeps us in business. if we did not have that we would not still be here. >> always been very involved in the community. from small things, sort of a ticket agent for a lot of activities in town, everything from school placed a chamber orchestra. we sought tickets. so we have become a supporter of the arts in that light, which also brings a lot of people and to talk to us. but we are also, you know, on local boards and involved with the local downtown organization. we are involved with local schools and supporting activities they have to be some of it is monetary, and some of it is just helping out.
5:56 pm

we are definitely reliant on the community. the writing, the readers, the writers, the people who support independence stores. there is a great writing community in vermont. we have the vermont college of fine arts turned up the street that has writing programs for both adults and children in creative writing. in so the first place customers go when they come in is our best seller table which is right up front. the independent booksellers best-seller list. this is a survey of independent booksellers across the country. not the same, although there is some overlap, but it's what independent booksellers is selling the most of. people go straight there into the new releases table and then they go right over the out of nowhere. does not have a big publisher, this level of publicity. we definitely rely on local
5:57 pm

light is to keep the things vibrant and interesting around here. you will see a lot of local authors on our front table on display. we also work with the local college when they have visiting professors in and they have residency programs that come and . very good writing. very powerful. >> a good number of our best sellers. each staff member as customers. it you can't recreate that, an algorithm on line. it's not the same thing is talking to people and having somebody say to my left it because i think you're going to love it because of this. you can't get that other places. i think the challenge to an outing in independent bookstore
5:58 pm

these days is definitely competition from the internet, both from online marketplace and the whole e-book, he-reader phenomenon that is very popular and definitely affects us. a lot of people, all of our regular customers, like a said, they love us, the supporters, but then they're like, yeah, i got this back. i got an ipad command it so easy to get a book. we definitely lost customers the way. a lot of people will buy e-book from mostar website, which we have enabled. not everybody does. we have lost customers that way. we don't lose customers to so much as they don't buy as much as they used to. we see a lot of the same people. the purchases may be and not as high as they used to be. it is a constant question, how are we going to survive in this new environment. publishing, and allow the
5:59 pm

bookstores are in precarious positions. it is something we think about all the time. there is now resting on our laurels, even if you been here almost 40 years. we are constantly trying to change and adapt and stay on top of things. adding e-books to our website. having a website that you can order any kind of books on. something we work on all the time. leon facebook. we bring in new products all the time. we have nonbook items that people really enjoyed. we definitely have to stay on top of things and make sure we are checking the next place we should be going and not just assuming that they will keep coming. it is very important to keep the bookstores because where you going to browse? book stores close, there is not going to be, you know, by stores going away to some extent, certainly for books. where are you going to brow,
107 Views
IN COLLECTIONS
CSPAN2 Television Archive
Television Archive  Television Archive News Search Service
Television Archive News Search Service 
Uploaded by TV Archive on
